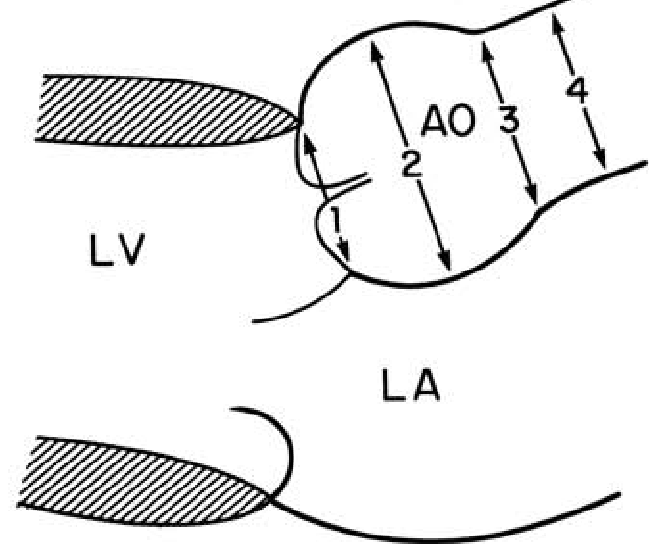
Evaluation of Aortic Diameters from Left Ventricular Outflow Tract (LVOT) View
In the LVOT view, the aortic (AO) diameters at the level of aortic valve annulus, the widest point of the AO sinuses, and the sinotubular junction are measured (Davis et al., 2014).
Two patterns of dilatation were found: dilatation occurring purely or predominantly at the level of the sinuses of Valsalva (type 1) and dilatation extending from the sinuses of Valsalva into the proximal ascending aorta (type 2).
Roman, M. J., Devereux, R. B., Niles, N. W., Hochreiter, C., Kligfield, P., Sato, N., Spitzer, M. C., & Borer, J. S. (1987). Aortic Root Dilatation as a Cause of Isolated, Severe Aortic Regurgitation: Prevalence, Clinical and Echocardiographic Patterns, and Relation to Left Ventricular Hypertrophy and Function. Annals of Internal Medicine, 106(6), 800–807. https://doi.org/10.7326/0003-4819-106-6-800
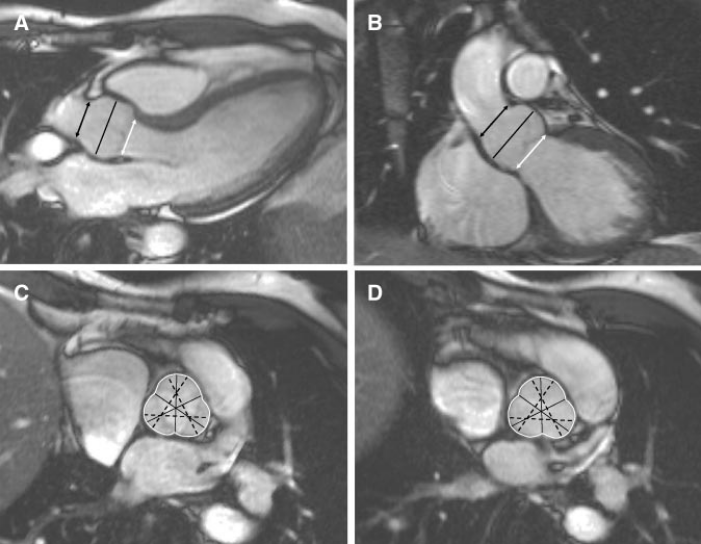
The levels of annulus, sinus, and sinotubular junction measurements (white arrow, black line, and black arrow, respectively).
Burman, E. D., Keegan, J., & Kilner, P. J. (2008). Aortic Root Measurement by Cardiovascular Magnetic Resonance: Specification of Planes and Lines of Measurement and Corresponding Normal Values. Circulation: Cardiovascular Imaging, 1(2), 104–113. https://doi.org/10.1161/CIRCIMAGING.108.768911
CoA accounts for 5-8% of CHD.[13] Isolated forms occur in less than half of the patients, CoA is often found in combination with BAV and mitral valve anomalies. It is usually sporadic, but genetic influences can play a role: There is a male predominance of 1,5-1,7/1, and 10-15% of Turner syndrome patients have aortic CoA.[14]
The BAV is the most frequent congenital cardiac malformation, with a prevalence of 1-2% in the general population. Concomitant aortic dilatation is seen in 80% of patients.[19] Three valve morphologies have been identified: Type I (the most prevalent, 69-85%) has a fusion of right and left coronary cusps, type II is fusion of right and non-coronary cusps, and type III (the least prevalent) shows fusion of the left and non-coronary cusp.
TOF is the most common form of cyanotic CHD and accounts for 10% of all congenital heart defects. Dilatation of the proximal aorta is a common feature in patients with unrepaired TOF and PA/VSD, which can already be observed at fetal echocardiography. The aorta in TOF is dilated mainly at the root, tapering down towards the ascending aorta; the aortic arch is usually of normal size.
Francois, K. (2015). Aortopathy associated with congenital heart disease: A current literature review. Annals of Pediatric Cardiology, 8(1), 25. https://doi.org/10.4103/0974-2069.149515