Atrial function
Feature summary
Atrial total emptying fraction
Reservoir-to-minimum-volume change expressed as a percentage of maximum atrial volume.
Family: functionalUnit family: %Source: Cine long-axis CMRPrimary output group: Atrial emptying fractionsHeart failure (I50)Atrial fibrillation and flutter (I48)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.LA conduit and booster fractions
ECG-timed separation of LA passive emptying and active atrial contraction.
Family: functionalUnit family: %Source: Cine long-axis CMR plus ECG timingPrimary output group: LA phasic functionDiastolic heart failure (I50.3)Hypertrophic obstructive cardiomyopathy (I42.1)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.Atrial expansion index
Maximum-to-minimum atrial volume change normalized to minimum volume.
Heart failure (I50)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.LA peak emptying rates
Early and late negative derivative extrema of the smoothed LA volume curve, reported as positive magnitudes.
Family: functionalUnit family: mL/sSource: Cine long-axis CMR volume curvePrimary output group: LA emptying ratesHypertrophic obstructive cardiomyopathy (I42.1)Diastolic heart failure (I50.3)Disease badges are literature-context navigation only; not diagnoses, CardiacNexus classifiers, or validated phenotype-to-ICD associations.
Atrial function phenotypes describe reservoir, conduit, and booster-pump behavior from the same long-axis atrial volume curves used by Atrial structure. This page documents CardiacNexus current output behavior; it does not define diagnostic thresholds for atrial fibrillation, heart failure, or diastolic dysfunction.
- Modality
- Cine long-axis CMR
- UKB source
- Data Field 20208 plus ECG timing when available
- Pipeline step
- Long-axis atrial volume curve extraction and derivative analysis
- Outputs
- atrial_volume.csv, timeseries/atrium.npz, atrial volume/rate QC plots
- Maturity
- Source-audited phenotype page
Clinical question
Clinicians use atrial function to interpret whether an enlarged or normal-sized atrium has impaired reservoir, conduit, or booster-pump performance. LA emptying fraction and phasic function are discussed in CMR and echocardiography literature as markers of atrial remodeling, diastolic dysfunction, and prognosis, but CardiacNexus outputs are quantitative research phenotypes rather than classifiers [1] [2].
Anatomical and physiological definition
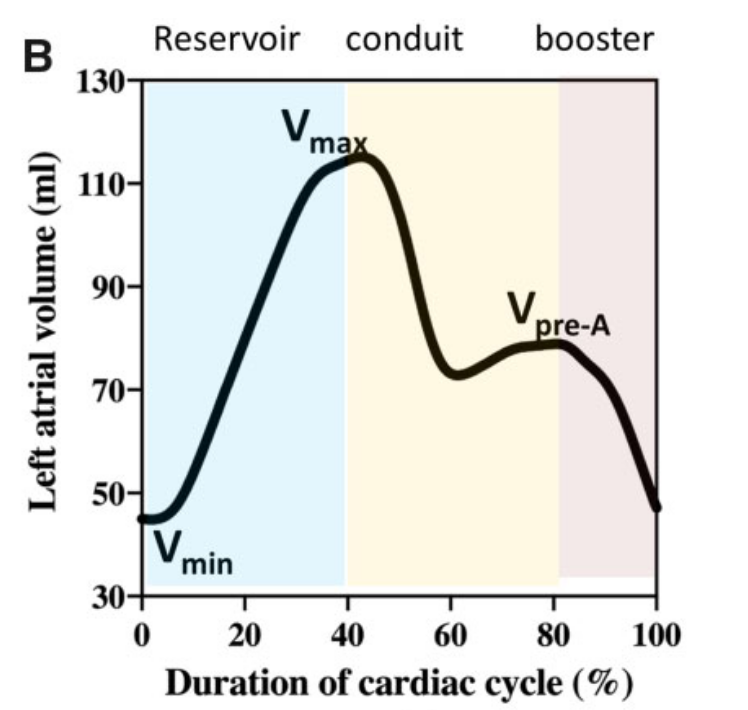
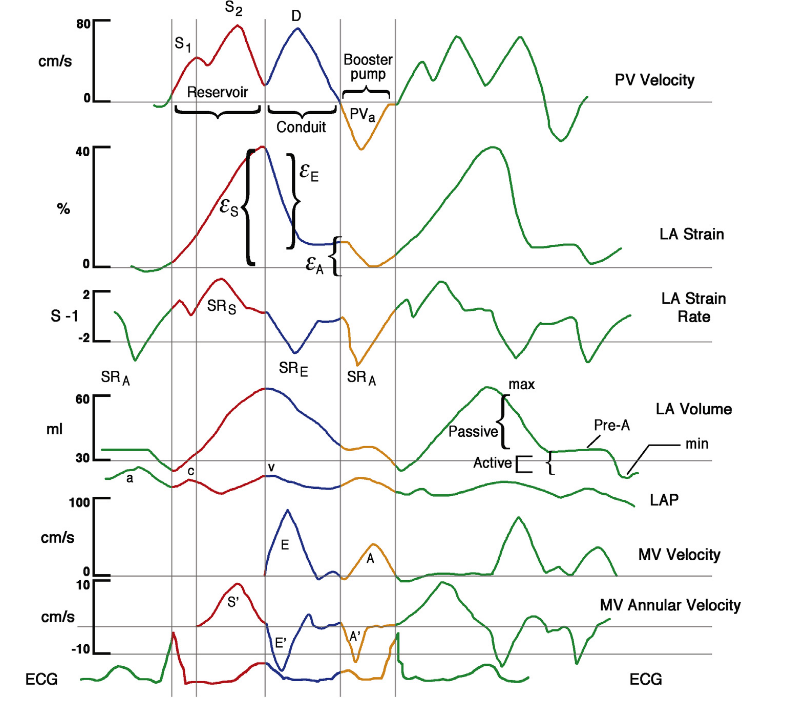
Reservoir function reflects atrial filling while the ventricle contracts and the mitral/tricuspid annulus descends. Conduit function reflects passive emptying into the ventricle during early diastole. Booster-pump function reflects active atrial contraction late in diastole when sinus rhythm and timing information allow that phase to be identified [1].
Source acquisition and UKB field
The current extraction uses UK Biobank cine long-axis CMR, UK Biobank Data Field 20208, plus resting ECG-derived timing when the pre-atrial-contraction frame is needed. Required image inputs and segmentation boundary assumptions are inherited from the atrial structure pipeline.
What exactly CardiacNexus measures
The functional rows use the same biplane LA and 4ch RA volume curves documented on the atrial-structure page. Indexed values require query_BSA(subject). Conduit and booster rows additionally require an ECG-derived T_pre_a that passes implementation timing checks.
Total emptying fraction
CardiacNexus computes LA and RA total emptying fraction from maximum and minimum framewise atrial volume:
Copyable formula
EF_total = (V_max - V_min) / V_max * 100Conduit and booster fractions
When ECG-derived pre-atrial-contraction timing passes checks, CardiacNexus records LA: V_pre_a [mL] and separates LA passive/conduit and active/booster components:
Copyable formula
EF_conduit = (V_max - V_pre_a) / V_max * 100Copyable formula
EF_booster = (V_pre_a - V_min) / V_pre_a * 100Atrial expansion index
The expansion index uses the same extrema but normalizes by minimum volume:
Copyable formula
EI = (V_max - V_min) / V_min * 100Peak emptying rates
For LA peak emptying rates, the implementation smooths the LA biplane volume curve, differentiates it, finds two negative derivative extrema, and reports their absolute values as PER-E and PER-A. The ratio LA: PER-E/PER-A is skipped when the implemented outlier guard detects an extreme value.

Output columns and units
| Display family | Exact output column | Unit | Status | Schema note |
|---|---|---|---|---|
| LA total emptying | LA: Total SV (bip) [mL] | mL | current | LA maximum minus minimum biplane volume |
| LA total emptying | LA: EF_total [%] | % | current | Reservoir summary from LA biplane extrema |
| RA total emptying | RA: EF_total [%] | % | current | Uses the current RA 4ch volume curve despite the legacy NPZ label |
| Expansion index | LA: EI [%] | % | current | Maximum/minimum volume based |
| Expansion index | RA: EI [%] | % | current | Maximum/minimum volume based |
| LA peak emptying | LA: PER-E [mL/s] | mL/s | current when derivative QC passes | Reported as a positive magnitude |
| LA peak emptying | LA: PER-A [mL/s] | mL/s | current when derivative QC passes | Reported as a positive magnitude |
| LA peak emptying indexed | LA: PER-E/BSA [mL/s/m^2] | mL/s/m² | current when BSA and PER pass | BSA-dependent |
| LA peak emptying indexed | LA: PER-A/BSA [mL/s/m^2] | mL/s/m² | current when BSA and PER pass | BSA-dependent |
| LA peak emptying ratio | LA: PER-E/PER-A | unitless | conditional current output | Outlier guard may skip the ratio |
| LA pre-atrial contraction | LA: V_pre_a [mL] | mL | conditional current output | Requires ECG-derived timing |
| LA pre-atrial contraction indexed | LA: V_pre_a/BSA [mL/m^2] | mL/m² | conditional current output | Requires ECG-derived timing and BSA |
| LA active function | LA: EF_booster [%] | % | conditional current output | Also called active EF in implementation comments |
| LA passive function | LA: EF_conduit [%] | % | conditional current output | Also called passive EF in implementation comments |
Output reconciliation
| Evidence layer | Result |
|---|---|
| Implementation source | 14 atrial-function outputs documented here: total emptying, expansion index, LA peak emptying rates, ECG-timed pre-atrial volume, conduit fraction, and booster fraction |
| Output inventory | docs/data/output_column_inventory.yml includes the same 14 outputs under atrial_volume.functional_columns |
| Phenotype dictionary | docs/data/phenotype_dictionary.yml links the same 14 outputs to this page |
| Page output table | all 14 output labels are listed above |
Required upstream inputs
la_2ch.nii.gz,la_4ch.nii.gz,seg_la_2ch.nii.gz, andseg_la_4ch.nii.gz.- The atrial structure volume curves and
timeseries/atrium.npz. - BSA lookup for indexed values.
- Resting ECG XML and successful timing checks for
T_pre_a, conduit, and booster outputs.
Reference ranges with cohort and method context
| Feature | Source | Cohort | Reference value | Status | Note |
|---|---|---|---|---|---|
| LA emptying fraction and phasic function | Hoit 2014 and CMR atrial function reviews [1] [2] | adult CMR/clinical review context | study-specific | Verified context source | Useful for interpretation, not a CardiacNexus-specific normal limit |
| Biplane LA volume and phasic function | Wandelt et al. CMR biplane/Simpson comparison [3] | CMR method-comparison cohort | method-dependent | Verified context source | Phase definitions and boundary conventions differ across studies |
| UKB CMR chamber context | Petersen et al. UK Biobank CMR reference ranges [4] | UK Biobank CMR reference cohort | structural context only | Verified context source | Functional atrial rows remain verification-queued |
Source-located registry status: docs/data/reference_range_sources.yml records Hoit 2014, Wandelt 2017, and Petersen 2017 as verified context sources for atrial-function interpretation, but the functional atrial rows remain verification-queued rather than promoted numeric normal ranges. This page therefore treats LA/RA emptying fractions and PER/PFR as method-dependent physiology context until row-level source tables and CardiacNexus phase definitions are adjudicated.
Disease interpretation
Reduced atrial emptying fraction and altered phasic function are discussed as markers of atrial remodeling, AF substrate, HFpEF/diastolic dysfunction, and HCM-related loading abnormalities [1] [2]. These disease badges are navigation context only. They do not indicate that CardiacNexus diagnoses AF, HF, or HCM from atrial function alone.
QC caveats and maturity boundary
Atrial function inherits segmentation, landmark, and volume-curve errors from the atrial structure pipeline. PER values are sensitive to temporal resolution, smoothing, arrhythmia, and noisy masks. Conduit and booster outputs are conditional: missing or rejected ECG timing leads to missing conditional outputs rather than imputed values.
Implementation provenance
Current outputs are implemented in src/feature_extraction/Long_Axis_20208/eval_atrial_volume.py.
| Feature family | Formula or computational route | Exact output columns | Source code file and function | Upstream dependencies | Conditional behavior | QC artifacts | Schema debt |
|---|---|---|---|---|---|---|---|
| Total emptying and expansion | extrema of LA biplane and RA 4ch volume curves | LA: Total SV (bip) [mL], LA: EF_total [%], RA: EF_total [%], LA: EI [%], RA: EI [%] | eval_atrial_volume.py; base feature update and EI blocks | la_2ch.nii.gz, la_4ch.nii.gz, seg_la_2ch.nii.gz, seg_la_4ch.nii.gz | subject skipped if long-axis inputs or segmentation fail | timeseries/atrium.npz, atrial volume QC plots | RA volume uses 4ch route despite legacy (bip) NPZ label |
| LA peak emptying rates | smoothed LA biplane volume derivative; two negative extrema reported as positive magnitudes | LA: PER-E [mL/s], LA: PER-A [mL/s], LA: PER-E/BSA [mL/s/m^2], LA: PER-A/BSA [mL/s/m^2], LA: PER-E/PER-A | eval_atrial_volume.py; PER derivative block | LA biplane volume curve, temporal resolution, BSA lookup | rows skipped if derivative fitting, peak checks, BSA, or ratio guard fails | atrial PER/time-series QC plot | PER values are derivative-derived and smoothing-sensitive |
| ECG-timed pre-atrial contraction | resting ECG timing converted to cine frame and checked against volume-curve landmarks | LA: V_pre_a [mL], LA: V_pre_a/BSA [mL/m^2], LA: EF_booster [%], LA: EF_conduit [%] | eval_atrial_volume.py; pre-atrial-contraction block | resting ECG XML timing, temporal resolution, LA biplane curve, BSA lookup | rows skipped if ECG timing is missing, outside frame range, or inconsistent with curve landmarks | LA: T_pre_a in timeseries/atrium.npz; ECG/time-series QC plot | conditional outputs require sinus-timing assumptions and external ECG availability |
Source audit
- Formula claims were checked against the current implementation strings and update blocks in
eval_atrial_volume.py. - Full atrial-function output coverage was reconciled across the implementation contract, page text,
docs/data/output_column_inventory.yml, anddocs/data/phenotype_dictionary.yml. docs/data/reference_sources.ymlexists and is used here as the current curated reference-source registry for scientific and implementation source metadata.- One LA peak emptying rate curve figure is displayed from a page-local public path and registered in
docs/data/figure_provenance.yml; permission and exact source-panel review remain pending for draft use.
Related pages
References
- Hoit BD. Left atrial size and function: role in prognosis. Journal of the American College of Cardiology. 2014;63(6):493-505. doi:10.1016/j.jacc.2013.10.055. PMID:24291276.
- Peters DC, Lamy J, Sinusas AJ, Baldassarre LA. Left atrial evaluation by cardiovascular magnetic resonance: sensitive and unique biomarkers. European Heart Journal - Cardiovascular Imaging. 2021;23(1):14-30. doi:10.1093/ehjci/jeab221. PMID:34718484; PMCID:PMC8685602.
- Wandelt LK, Kowallick JT, Schuster A, Wachter R, Stumpfig T, Unterberg-Buchwald C, Steinmetz M, Ritter CO, Lotz J, Staab W. Quantification of left atrial volume and phasic function using cardiovascular magnetic resonance imaging: comparison of biplane area-length method and Simpson's method. The International Journal of Cardiovascular Imaging. 2017;33(11):1761-1769. doi:10.1007/s10554-017-1160-9. PMID:28523471.
- Petersen SE, Aung N, Sanghvi MM, Zemrak F, Fung K, Paiva JM, Francis JM, Khanji MY, Lukaschuk E, Lee AM, Carapella V, Kim YJ, Leeson P, Piechnik SK, Neubauer S. Reference ranges for cardiac structure and function using cardiovascular magnetic resonance in Caucasians from the UK Biobank population cohort. Journal of Cardiovascular Magnetic Resonance. 2017;19(1):18. doi:10.1186/s12968-017-0327-9. PMID:28178995; PMCID:PMC5304550.
- Aquaro GD, Pizzino F, Terrizzi A, Carerj S, Khandheria BK, Di Bella G. Diastolic dysfunction evaluated by cardiac magnetic resonance: the value of the combined assessment of atrial and ventricular function. European Radiology. 2019;29(3):1555-1564.